Migraine Rules 2024
Migraine is present in 12% of the world’s population and in 25% of women and 6% of men. It is a severe, disabling, medical condition that often leads to evaluation in the emergency room.
Like treating any neurologic problem, there is a way to go about treating Migraine. What is it? How do you treat Migraine headaches? What are the rules? The mean looking teacher in the thumbnail knows what to do and is strongly advising her students all about the rules.
This is an article by Britt Talley Daniel MD, retired member of the American Academy of Neurology, the American Headache Society, migraine textbook author, podcaster, YouTube video producer, and blogger.
Migraine Rules: Treat at onset of the headache. Take the right kind of drug. Take enough of the right drug.
Treat at Onset.
This means that all medication should be taken at the very first beginning of the headache. Don’t wait, thinking it’s not going to be “one of those” when it very well may be--a bad Migraine coming on.
Migraine headaches may start in the back of the head and move forward behind an eye. Treat it while it is in the neck.
Migraine without aura headaches may also start in the forehead, eye, or cheek area. This is not sinus headache unless there is green or yellow nasal discharge or pus on a CAT scan of the sinuses---treat it as a migraine.
Usually Migraine with aura attacks occur minutes before the headache part starts and then Migraine should be treated at the onset of the aura. Sometimes the aura, which is usually visual, comes on in the middle or end of the Migraine and in that situation the patient should treat at the onset of the headache.
All the generic oral triptans except, naratriptan and frovatriptan, work in 30 minutes, and should be used. These are: Imitrex (sumatriptan), Zomig (zolmitriptan), Maxalt (rizatriptan), Relpax (Eletriptan), or Axert (almotriptan.
Frova (frovatriptan) and Amerge (naratriptan) take 1-2 hours to start working and are mainly used for menstrual migraine.
Eighty percent of migraine patients may be pain free at two hours if they treat at onset. Triptans block the release of neurochemical inflammatory drugs which come at 20-40 minutes into a Migraine.
Triptans are the universal best drugs for acute therapy for migraine. However, twenty percent of patients don’t respond to Triptans and other treatment options must be pursued. Triptans also have reasons not to be taken by certain patients. These are called contraindications and are uncontrolled hypertension, history of angina, heart attack, cerebrovascular disease, or basilar/hemiplegic Migraine.
Since 2020 there are 3 new acute therapy drugs for Migraine which have no cardiac/cerebral problem and might work for the 20% of triptan non-responders. However, these drugs are name brand and more expensive than universally generic triptans.
They don’t work as well as triptans do but are worth trying. These 3 drugs are Nurtec ODT 75, Ubrevly, and Reyvow.
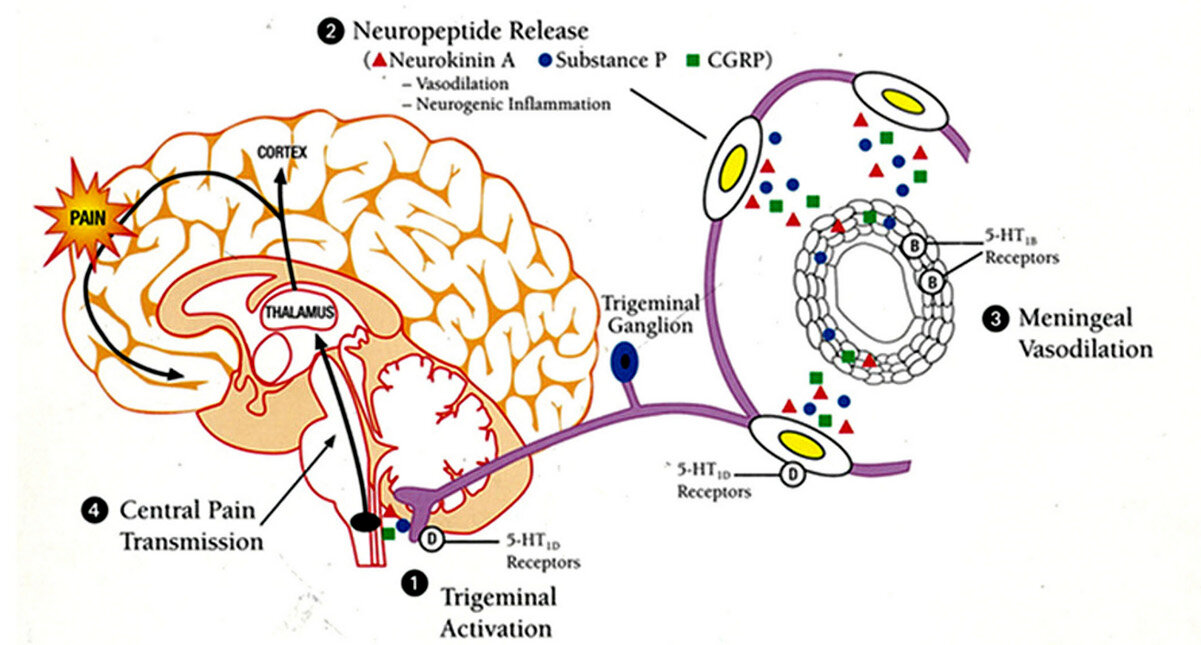
The Migraine Timing Cycle. Take triptan at 1, to stop neuropeptide release at 2
Triptans came out in 1991 with the introduction of subcutaneous Imitrex (sumatriptan). Now there are 7 different triptans available and they are all generic. The fastest triptans are injectable SC sumatriptan and nasal spray zolmatriptan which both work in 10 minutes.
Take The Right Drug.
In general, for severe migraine patients this is going to be a Triptan. It is true that many patients with mild migraine can treat their headache with Excedrin, or an NSAID like ibuprofen or naproxen, but the severe headache patients—the type that end up in the Doctor’s Office or the ER—will usually need a Triptan.
Read my Mini Migraine Book Here
Usually the Triptans will treat the whole migraine syndrome—headache, nausea, vomiting, photophobia, sonophobia—and they work best if taken at onset of headache. After the Migraine process starts in the brain arterial dilatation starts 20-40 minutes later. Triptans cause the cerebral arteries to constrict and need to be in the working before the end of 40 minutes to work.
It is said that triptans will improve a Migraine if taken anywhere in the course of the attack. That’s improvement of headache, not headache free-all symptoms gone, which only happens when the triptan is taken at onset of the Migraine.
I have instructed innumerable Migraine headache patients about this, usually when they tried a triptan from another doctor that the patient said didn’t work, because they treated late. Then on return to the office later those same Migraine patients were very surprised and grateful for how their triptan performed when taken early.
Take enough of the right drug.
This is a dosing situation which varies from patient to patient. Elephant rifle load (the biggest gun) for Migraine remains injectable Imitrex (sumatriptan) 6 mg sc which works the fastest, in 10 minutes, and gives the highest level of 100 mg in the brain. Nasal spray triptans-sumatriptan and zolmitriptan-work in 10 minutes but give a dose of 10 mg in the brain, while the oral triptans work in 30 minutes and give a brain dose of 30 mg.
The answer of which triptan the patient will take is a discussion between patient and doctor. Most persons want to take a pill first, nasal spray next, and subcutaneous injection last. Many persons do not want needle injection treatment and I respect that.
Usually in that situation if I use sumatriptan and it works with their insurance, I will suggest the large 100 mg dose which has a small risk of increased side effects. The same high dose of 5 mg is a good start for zolmitriptan but all the other 5 triptans only have one dose size offered.
Many times adding 2 Aleve (200 mg) to the triptan the patient uses will add effective treatment results. To be clear then, as a example, at onset the migraineur would take 1 100 mg sumatriptan, and 2 200 mg Aleve, which they may repeat once only in 24 hours.
To avoid medication overuse syndrome triptans should be limited to treatment of 2 days a week where the patient may take 1-2 sumatriptan tablets each day. That week the patient would take 4 100 mg sumatriptan tablets on 2 days only. It is the number of treatment days that is important, not the number of pills.
I have seen innumerable Migraine patients in referral who got their triptan from the regular doctor and then started taking it once or twice a day every day for a month and who came to see me for daily Migraines. They had developed medication overuse headache by not limiting their triptan therapy.
Read my article on “Medication Overuse Headache” on my website, www.doctormigraine.com.
Oral Imitrex (sumatriptan) 25, 50, 100 mg
Treximet (sumatriptan/naproxen) 1 tablet
Maxalt (rizatriptan), 5, 10 mg
Zomig (zolmitriptan) 2.5,5.0 mg
Axert (almotriptan) 12.5 mg
Relpax (eletriptan) 40 mg
Amerge (naratriptan) 2.5 mg
Frova (frovatriptan) 2.5 mg may be tried at onset of the headache.
Check out my Big Migraine Book Here.
This site is owned and operated by Internet School LLC, a limited liability company headquartered in Dallas, Texas, USA. Internet School LLC is a participant in the Amazon Services LLC Associates Program, an affiliate advertising program designed to provide a means for sites to earn advertising fees by advertising and linking to Amazon.com. Although this site provides information about various medical conditions, the reader is directed to his own treating physician for medical treatment.
All the best.
Follow me at: www.doctormigraine.com, Pinterest, Amazon books, Podbean, and YouTube.
Britt Talley Daniel MD